Friday, December 20, 2019
Monday, December 16, 2019
Hospital Groups Sue Trump Administration Over Pricing Transparency Rule
On Wednesday, Dec. 4, 2019, four major hospital
groups filed a lawsuit against the Trump administration
to challenge the Nov. 15, 2019, final rule that would
require hospitals to disclose their pricing information,
including negotiated rates.
The Federation of American Hospitals, the American Hospital Association, the Association of American Medical Colleges, the Children’s Hospital Association and three hospitals filed the suit in the U.S. District Court for the District of Columbia, stating that the Centers for Medicare and Medicaid Services (CMS) exceeded their authority with the rule. The lawsuit also states that the pricing disclosure rule violates the First Amendment.
What’s included in the final rule?
Under the rule, hospitals are now required to provide easily accessible billing information to patients by Jan. 1, 2021. This means having all standard charges available online and in one single data file that can be “read by other computer systems,” according to a CMS press release.
The charges listed would include “the gross charges, payer-specific negotiated charges, the amount the hospital is willing to accept in cash from a patient, and the minimum and maximum negotiated charges,” to the release. Hospitals that fail to comply with the rule’s requirements would face a $300 per day civil penalty.
The hospital groups’ lawsuit contends that requiring hospitals to publish the different charges, including their privately negotiated prices with insurers, “will confuse patients and unduly burden hospitals.”
We will continue to monitor any developments regarding this lawsuit and will provide updates as necessary.
The Federation of American Hospitals, the American Hospital Association, the Association of American Medical Colleges, the Children’s Hospital Association and three hospitals filed the suit in the U.S. District Court for the District of Columbia, stating that the Centers for Medicare and Medicaid Services (CMS) exceeded their authority with the rule. The lawsuit also states that the pricing disclosure rule violates the First Amendment.
What’s included in the final rule?
Under the rule, hospitals are now required to provide easily accessible billing information to patients by Jan. 1, 2021. This means having all standard charges available online and in one single data file that can be “read by other computer systems,” according to a CMS press release.
The charges listed would include “the gross charges, payer-specific negotiated charges, the amount the hospital is willing to accept in cash from a patient, and the minimum and maximum negotiated charges,” to the release. Hospitals that fail to comply with the rule’s requirements would face a $300 per day civil penalty.
The hospital groups’ lawsuit contends that requiring hospitals to publish the different charges, including their privately negotiated prices with insurers, “will confuse patients and unduly burden hospitals.”
“CMS' final rule fails to offer patients easy-to understand information regarding their out-of pocket obligations for care -- so we feel obligated to contest the regulation. We contend the agency exceeded its authority and should go back to the drawing board.” - Chip Kahn, chief executive of the Federation of American HospitalsWhat’s next?
We will continue to monitor any developments regarding this lawsuit and will provide updates as necessary.
Thursday, September 19, 2019
California is Burning $80,665 on Healthcare for One Employee Per Year
Honestly, I have no clue how that is even possible. The annual cost of healthcare for one person per year should be between $6,000 and $9,000. California's state average is $9,500. Yet we have a plethora of "public servants" costing the state over $50,000 per year. Yet another example as to how taxpayer dollars are flat-out abused and wasted by elected officials and bureaucrats. These amounts are so absurdly high, it is hard to imagine how this could happen without rampant fraud.
This is from the OC Register:
One of the most generous health insurance plans enjoyed by a California public servant last year — costing $80,665 — went to a communications manager for the obscure Water Replenishment District of Southern California.
At the embattled Los Angeles Department of Water and Power — raided by the FBI in July, and yet to produce documents detailing how a worker earned $313,865 in overtime pay — there were 153 workers with health plans costing $57,816 each.
In Riverside County’s Rubidoux Community Services District, the general manager received health benefits totaling $55,717. In San Bernardino County’s Cucamonga Valley Water District, the general manager’s health benefits cost $38,191 to cover his family. In Anaheim, 31 workers — mostly in public safety — had health plans costing more than $36,000 each.
A new analysis of public spending on employee health insurance by Transparent California — whose findings were mirrored by the Southern California News Group’s own data crunching — found that workers toiling in California’s cities, counties, special districts and state offices received health benefits costing about 50 percent more than the average in California, which is $9,476.
And, surprisingly often, benefits cost two, three, four, up to even eight times as much.
“Spending over $50,000 on a single employee’s health insurance plan is an inexcusable waste of taxpayer funds,” said Robert Fellner, executive director of Transparent California, in a statement.
“Medical plans this expensive simply don’t exist in the broader market, which is a strong indication that providers are exploiting the fact that these governments are happy to pay inflated prices with other people’s money.”
California’s “wildly inflated health costs” bleed some $3.3 billion from taxpayers each year, Fellner calculated. ...
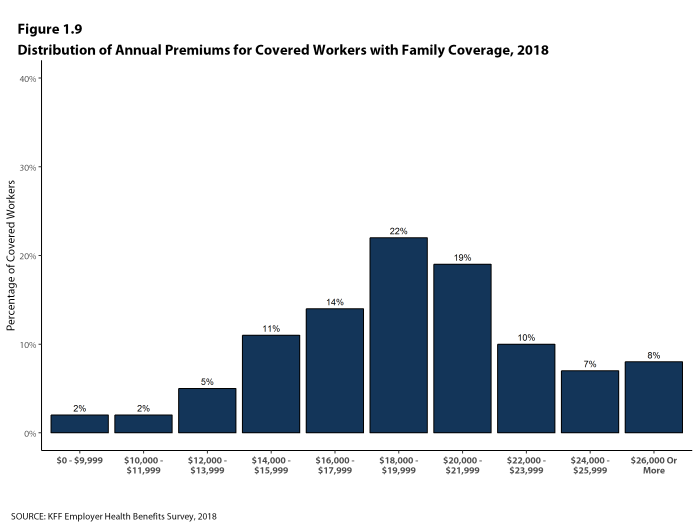
And a recent survey from the Kaiser Family Foundation found that 92 percent of family medical plans cost less than $26,000....
Nationwide, workers contribute one-third of their health care premiums, according to UBA’s data. In California, government workers pay an average of 23.3 percent.
But the Water Replenishment District of Southern California — like many public agencies here — doesn’t ask workers to pay anything.
The district not only picks up 100 percent of premiums for workers and their dependents, but also gives them an “IRS qualified health reimbursement account” for out-of-pocket expenses of $8,196 per worker and $4,928 per dependent. Each year.The full story is definitely worth your time to read.
Unused funds roll over for three years, then revert to the district. ...
Monday, September 16, 2019
Wednesday, September 11, 2019
Thursday, August 29, 2019
Book Review - Heaven on Earth: The Rise, Fall, and Afterlife of Socialism
The very first Armstrong & Getty Book Club (or A&G Book Review, TBD) has convened. Jack & Joe were joined by "Tim The Lawyer" Sandefur and "Craig the Healthcare Guru/Gangsta" Gottwals. The group sat down at the A&G Radio Ranch for the first in a series of podcasts in which each participant shared their thoughts on "Heaven on Earth: The Rise, Fall, and Afterlife of Socialism" by Joshua Muravchik.
Listen to us discuss:
- The difference socialism and fascism
- Why communism will always lead to fascism
- What leads folks to desire socialism
- The work ethic of Karl Marx
- Did you bring enough gum for everyone?
- And more
Thursday, August 1, 2019
Trump And The Senate Make Significant Progress On Hospital Price Transparency w/Armstrong & Getty
From Forbes:
On July 30, the Centers for Medicare and Medicaid Services proposed a landmark new rule that would require hospitals to make public, in a machine-readable format, prices “for all items and services provided by the hospital.” Critically, the rule would require hospitals to publish both their “gross charges,” or their sticker prices, along with “payer-specific negotiated charges,” or the prices hospitals negotiate with each insurer they work with.
In addition, the proposed rule would require hospitals to disclose “payer-specific negotiated charges for common shoppable services in a manner that is consumer friendly.” For example, hospitals would have to post what they charge for MRI scans and common lab tests that patients often pay for out-of-pocket.Full story.
“This proposal is now the most significant step any President has ever taken to deliver transparency and put patients in control of their care,” said Health and Human Services Secretary Alex Azar. He’s right. This rule, if finalized, will revolutionize the market for hospital care.
See also:
- CMS Takes Bold Action to Implement Key Elements of President Trump’s Executive Order to Empower Patients with Price Transparency and Increase Competition to Lower Costs for Medicare Beneficiaries.
- Fact Sheet: CY 2020 Medicare Hospital Outpatient Prospective Payment System and Ambulatory Surgical Center Payment System Proposed Rule (CMS-1717-P)
- Full Proposed Regulation: Medicare Program: Proposed Changes to Hospital Outpatient Prospective Payment and Ambulatory Surgical Center Payment Systems and Quality Reporting Programs; Price Transparency of Hospital Standard Charges; etc.
Thursday, June 20, 2019
Medicare For All? A False Sense Efficiency with Armstrong & Getty
As most of the folks running for President in 2020 profess their love for government provided healthcare and sing the siren song of “Medicare for All” you are likely to hear claims about Medicare’s efficiency and efficacy. Here are the facts they like to leave out:
- In 1965, government experts projected that in 1990, on an inflation-adjusted basis, Medicare would cost $12 billion. In reality, Medicare cost $107 billion in 1990.
- For nearly one-third of calls into the Medicaid/Medicare hotline reporting waste, fraud and abuse, government workers take over 4 months to begin investigation.
- Supporters like to point out that Medicare uses 98% of its funding on claims and only 2% on administration while private insurers generally spend 85% on claims and 15% on administration. This, they claim is superior efficiency. This fails to acknowledge the rampant fraud, misuse and abuse within Medicare.
- Independent experts tell us that as much as a third to half of all Medicare spending is improper or wasteful. Malcolm K. Sparrow, a professor at the Kennedy School of Government at Harvard University whose book License to Steal is a classic in the field, thinks that Medicare’s fraud-related losses may run “as high as 35%” of its budget.
- An infinitesimal amount of Medicare’s budget is spent on fraud detection, so yes, it is easy to get to 98% claim payment when 1 in every 3 claims you pay is fraudulent and you spend little to no time detecting fraud. The less effort Medicare takes to prevent fraud and the more money it lavishes on criminals, the more efficient it looks. (Source for these stats: "Overcharged: Why Americans Pay Too Much for Health Care" by Charles Silver, David A. Hyman Chapter 16.)
- In 2015, the outside contractors that handle bills for Medicare processed 1.22 billion claims. That’s almost 3.4 million claims per day.
- Medicare and Medicaid receive something like three billion claims a year. For a human being to spend five minutes reviewing each claim would require 125,000 people each working 2,000 hours a year. That’s not enough time to find and flag a fraud, much less to investigate one
- From 2009 to 2012, Medicare paid a total of $43 billion for durable medical equipment (DME). According to some reports, more than 60% of that amount—$25 billion plus—may have been paid out improperly. Unsurprisingly, DME suppliers lead the list of entities investigated for criminal health care fraud violations. But the federal government has recovered only about 3 percent of overpayment. (Source: Chapter 12 in Overcharged.)
- Medicare/Medicaid pay 80 cents on the dollar for services, forcing private plans to pay $1.30 for that same service.
- 65% of all healthcare is paid by taxpayers nationally, 70% in California.
- Medicare for all will cost an additional $32 Trillion over 10 years. Obamacare only costs $2T in comparison.
- Medicare is currently on pace to run out of money by 2026.
- US Spends $3.7 Trillion per year on health (today Medicare is just under a Trillion).
Wednesday, May 22, 2019
If You Like Your Deductible, You Can Keep Your Deductible ... Right After We Triple It
From Fierce Healthcare:
Health insurance deductibles have been steadily rising over the last decade, jumping 150% since 2009, according to an analysis by the Kaiser Family Foundation (KFF).
The report, published ahead of Deductible Relief Day on May 19, shows the average deductible for a single person in 2009 was $533. It was $1,350 in 2018.
The number of adults required to pay deductibles has gone up as well, the analysis found. In 2009, 59% of people on an employer plan were required to pay a deductible. That number was 85% in 2018.
Oof, How's That $2,500 Drop in Premiums for the Average Family Working Out?
From Modern Healthcare:

The Consumer Price Index for health insurance in April spiked 10.7% over the previous 12 months—the largest increase since at least April 2014, according to a Modern Healthcare analysis of the U.S. Bureau of Labor Statistics' unadjusted monthly Consumer Price Index data.

Tuesday, May 14, 2019
Generic Drugmakers Allegedly Inflated Prices Over 1,000% - 44 States Now Sue
60 Minutes blew the lid off of this unbelievable story here on Sunday night.
More on this story here:
It might be the biggest price-fixing scheme in U.S. history. On Friday, Connecticut and a coalition of more than 40 states filed a 500-page lawsuit accusing the biggest generic drug makers of a massive, systematic conspiracy to bilk consumers out of billions of dollars. It's a more sweeping version of a similar lawsuit the states filed in 2016 that's still being litigated. The generic industry vehemently denies the allegations.On Tuesday morning I went on the Armstrong and Getty show to explain what governmental changes created the environment where such an absurd ripoff could occur.
More on this story here:
- CNBC: Drugmakers allegedly inflated prices over 1,000% and 44 states are now suing
- Washington Post: States allege generic drug executives deleted texts, obstructed justice in price cartel probe
- USA Today: States: Drugmakers collude on generic price hikes, overcharge consumers and states billions
- Financial Post: Apotex among 20 generic drug firms accused of vast U.S. price-fixing scheme
Tuesday, April 16, 2019
Study: Wellness Programs "Don’t Cut Costs for Employers, Reduce Absenteeism or Improve Workers’ Wealth"
From Kaiser Health News:
Workplace wellness programs have become an $8 billion industry in the U.S. But a study published Tuesday in JAMA found they don’t cut costs for employers, reduce absenteeism or improve workers’ health.
Most large employers offer some type of wellness program — with growth fueled by incentives in the federal Affordable Care Act.
A host of studies over the years have provided conflicting results about how well they work, with some showing savings and health improvements while others say the efforts fall short.
Many studies, however, faced a number of limitations, such as failing to have a comparison group, or figuring out whether people who sign up for such wellness programs are somehow healthier or more motivated than those who do not.
Now researchers from the University of Chicago and Harvard may have overcome these obstacles with one of the first large-scale studies that is peer-reviewed and employs a more sophisticated trial design.
They randomly assigned 20 BJ’s Wholesale Club outlets to offer a wellness program to all employees, then compared results with 140 stores that did not.
The big-box retailer employed nearly 33,000 workers across all 160 clubs during the test.
After 18 months, it turned out that yes, workers participating in the wellness programs self-reported healthier behavior, such as exercising more or managing their weight better than those not enrolled.
But the efforts did not result in differences in health measures, such as improved blood sugar or glucose levels; how much employers spent on health care; or how often employees missed work, their job performance or how long they stuck around in their jobs.Full story.
Thursday, April 11, 2019
People Are Addicted to All Things Digital - And Yes, This Calls for Employer Accommodation
Pretty eye-opening piece from the folks over at Fisher Phillips:
... It is prudent to accommodate an individual with a digital addiction the same way you would accommodate any other individual: engaging in the interactive process, and reviewing and discussing any restrictions, limitations, or accommodations that may be needed. While there may be concerns regarding an employee’s ability to return to work in the digital age after receiving treatment for a directly related addiction, this concern cannot be used as a basis to engage in an adverse action against an employee.
This remains the case even if the disorder is not officially “diagnosable.” In other words, an employer must take a digital addiction seriously, even if it does not understand the addiction or personally believe the addiction is legitimate. ...
The law requires that you participate in a “good faith” interactive process, which means considering each and every possible reasonable accommodation in “good faith.” Document any legitimate reasons why an accommodation may not be “reasonable,” but understand that not everything is “unreasonable.” While employers do not have to provide accommodations that are unduly burdensome, “undue burden” is an extremely tough standard to meet and is looked at primarily in financial terms by courts. So, unless a particular accommodation costs you some serious money, results in a loss of serious money through disruption to your operations, or is a direct threat to the health and safety of others, you are probably going to have to provide it. ...
Friday, March 22, 2019
Best of March Compliance and Benefit News
|
|
Thursday, March 14, 2019
Spent the Morning with Armstrong & Getty to Discuss Woes & Cures in U.S. Healthcare
Saturday, March 9, 2019
Trump Administration Considers Groundbreaking Regulation Forcing Healthcare Providers to Disclose Secret Industry Pricing
This proposed regulation has the potential to do more for healthcare price containment and transparency than the 40,000 pages of statues and regulations spawned by the Patient Protection and Affordable Care Act ("PPACA" or "Obamacare"). The Trump Administration is considering a regulation to compel doctors, hospitals and other healthcare providers to make the "secret" agreements on pricing they have in place with the insurance industry publicly available. For the first time in the history of modern insured healthcare in America, the public would actually know the real prices and the free market would begin to be unleashed.
The U.S. Department of Health and Human Services (HHS) is seeking public comment on this proposed regulation. Absolutely everyone should take the time to make their views known here. As the Wall Street Journal Reports, "[t]he request for public comment has been largely overlooked because it was tucked into a 700-page draft regulation released last month on improving patients’ access to their electronic health records. Many insurers and hospital groups declined to discuss the government’s request for comment, saying they were still studying the idea."
See Footnote 1 (FN. 1) below for a copy of the comment I submitted to HHS on this regulation. Please use your own words as HHS does not want duplicate comments. This is solely provided so you can see the type of comment that may be appropriate if you agree with what you have read in this post. The relevant section of the regulations is reprinted below in FN. 2 for your convenience.
The Journal also reports:
Are there electronic mechanisms/processes available for providing price information to patients who are not registered (i.e., not in the provider system) when they try to get price information?
Should price information be made available on public websites so that patients can shop for care without having to contact individual providers, and if so, who should be responsible for posting such information? Additionally, how would the public posting of pricing information through API technology help advance market competition and the ability of patients to shop for care?
If price information that includes a provider's negotiated rates for all plans and the rates for the uninsured were to be required to be posted on a public website, is there technology currently available or that could be easily developed to translate that data into a useful format for individuals? Are there existing standards and code sets that would facilitate such transmission and translation? To the extent that some data standards are lacking in this regard, could developers make use of unstandardized data?
What technical standards currently exist or may be needed to represent price information electronically for purposes of access, exchange, and use?
Would updates to the CMS-managed HIPAA transactions standards and code sets be necessary to address the movement of price information in a standardized way?
What future requirements should the Department consider regarding the inclusion of price information in a patient's EHI, particularly as it relates to the amount paid to a health care provider by a patient (or on behalf of a patient) as well as payment calculations for the future provision of health care to such patient?
The U.S. Department of Health and Human Services (HHS) is seeking public comment on this proposed regulation. Absolutely everyone should take the time to make their views known here. As the Wall Street Journal Reports, "[t]he request for public comment has been largely overlooked because it was tucked into a 700-page draft regulation released last month on improving patients’ access to their electronic health records. Many insurers and hospital groups declined to discuss the government’s request for comment, saying they were still studying the idea."
See Footnote 1 (FN. 1) below for a copy of the comment I submitted to HHS on this regulation. Please use your own words as HHS does not want duplicate comments. This is solely provided so you can see the type of comment that may be appropriate if you agree with what you have read in this post. The relevant section of the regulations is reprinted below in FN. 2 for your convenience.
The Journal also reports:
'It’s an effort by the president to help put Americans back in control of price ata,' said Dr. Don Rucker, national coordinator for health information technology at the Department of Health and Human Services. 'Our interest is on how can we empower the American public to shop for their care and control it.' Industry officials say the administration faces many hurdles before implementing such price transparency. The move is likely to be met by fierce opposition, including possible legal challenges, from hospitals, doctors groups and insurers since it could have far-reaching impact.
I couldn't agree more. Insurers and providers alike will have a bullseye on the Trump Administration and the officials responsible for implementing this rulemaking. And that is no small lobby, with pockets as deep as one-fifth of the entire U.S. economy. The cash cow of obfuscation, secret discounts, unknown prices and third-party payment would begin a rather strict diet very soon if this information were permitted to flow into the light of day.
I can already imagine insurance plans with very large deductibles paired with massive HSA or HRA accounts and online shopping tools. This will allow patients to spend their own pre-tax healthcare dollars shopping on robust online comparison platforms telling you exactly what your shoulder MRI will cost at the 15 nearest providers. This can lead to the sort of consumerism in healthcare that we've only been partially able to achieve around the edges so far for procedures like Lasik eye surgery, vasectomies or cosmetic surgeries - areas where providers advertise pricing and patients regularly spend their own money.
What kind of arguments are made against this type of transparency and consumerism? Well, as it turns out, embarrassingly weak ones. Consider this one from the Journal's article, "[t]he American Hospital Association said it opposes the move. 'Disclosing negotiated rates between insurers and hospitals could undermine the choices available in the private market,' said Tom Nickels, an executive vice president of the trade group. 'While we support transparency, this approach misses the mark.'
I actually laughed out loud at this assertion. Yes, it certainly could "undermine choice," particularly in the short run as the most bloated, inefficient and overpriced providers are driven out of business for failing to be competitive. But when has true competition, price transparency and a free-market ever actually hurt the consumer, El Presidente Nicolás Maduro? This assertion isn't ground in reality. Consumer choice will explode as providers begin to compete on price, expensive providers become more efficient, and lower cost options spring up at your local drug or box stores. Then, Healthcare Guru's (like yours truly, thanks Armstrong & Getty) will get busy designing coverage that rewards consumers who shop for price by loading up pre-tax accounts and making online price comparison tools readily available.
The Journal further notes that:
Hospital groups also said the rule is unnecessary because they already publicly release their list prices. Hospitals had to comply with that new Trump administration requirement this year. But the steep discounts that insurers negotiate from the list prices remain kept from public view.
The only thing that matters in that quote is the last sentence. The prior sentences represent another anemic assertion by providers to try and keep their pricing scheme in the dark. No, we don't have to tell you the real prices because we've already published hard to find, unintelligible lists of completely fake prices that nobody ever pays!
In fact, insurers and providers regularly engage in contractual agreements not to disclose the prices they've negotiated as those prices are "proprietary." Yes, that's right, the price is proprietary. I cannot fathom a more un-American, anti-capitalistic circumstance than secret proprietary pricing. First, American workers pay these premiums with mostly hidden dollars as wages are suppressed to pay for year over year double-digit premium escalation. Then when they visit a doctor where they will be expected to pay 20% of the bill, patients are often not permitted to see the price until afterwards. What sort of insanity have we all signed up for here? How have we allowed to let this go on this long?
As the Journal story states:
The prices charged for health care vary widely depending on whether a provider is in or out of the patient’s insurance network and on the insurer’s undisclosed price agreements with hospitals. Employers and patients are often unable to see which hospital systems and doctor’s offices are driving prices upward. Some health-care economists argue that the secrecy is a factor in why the U.S. spends more per resident on health care than any other developed nation.
That last sentence is the understatement of 2019. I realize the year is young, but I cannot comprehend any healthcare economist that would argue that secrecy in pricing is not contributing to our astronomically high healthcare costs.
That this decades-long scam may now begin to crumble because we have a President in place who is so unconventional, bold and outside the norm of traditional party ties is both fitting and ironic. Yes, he is a billionaire businessman widely lauded by many in the business community for the country's current economic growth. But he's clearly not beholden to the $4 trillion dollar healthcare industry the way so many in both parties are. After sharing this story with my friends Jack and Joe of The Armstrong and Getty Radio Show, one of the first questions they asked me was which political party, if any, will support this? Maybe neither.
It will be captivating to see how this rolls forward politically. My suspicion is that the far left third of the Democrat Party will generally support this as a way to stick it to big insurance and giant hospital conglomerates; not because of any affinity for consumer-driven free-markets. I also think that the more libertarian leaning 20 to 30 percent of the Republican Party may support it as a warm embrace of cleaner capitalism and a strong shot across the bow of the crony capitalism that dominates the industry now. (See FN. 3 for more background on the legislative history giving rise to this regulation and FN 4 for my response to fellow free-marketers who may find it peculiar to see me arguing for more regulation.)
One thing we can be sure of is that any of our elected officials who receive substantial donations from the healthcare industry will come out against this as this threatens the very core of that system. And there are plenty in both parties in that camp. Maybe they won't actually come out against the regulation, as being out publicly loud and proud against telling someone the price before they buy something isn't a particularly good look; even for the most Marxist among us. But they will work vehemently during the regulatory sausage making to water down the strength of the rule and do all they can to render it impotent. For more on that, see my discussion as to how the Obama Administration wholly neutered PPACA's individual mandate once it realized it was going to start costing them votes to penalize those who didn't want to buy insurance.
One thing we can be sure of is that any of our elected officials who receive substantial donations from the healthcare industry will come out against this as this threatens the very core of that system. And there are plenty in both parties in that camp. Maybe they won't actually come out against the regulation, as being out publicly loud and proud against telling someone the price before they buy something isn't a particularly good look; even for the most Marxist among us. But they will work vehemently during the regulatory sausage making to water down the strength of the rule and do all they can to render it impotent. For more on that, see my discussion as to how the Obama Administration wholly neutered PPACA's individual mandate once it realized it was going to start costing them votes to penalize those who didn't want to buy insurance.
The full article from Stephanie Armour and Anna Wilde Mathews writing at the Wall Street Journal is worth your time to read. In the meantime, here are some other outstanding sections from their story:
FN. 1: Sample Comment to Proposed Regulation - The language in Section VIII., C, 3 of this proposed regulation found on pages 90-91 of the PDF requiring medical providers to disclose the true pricing of medical procedures is an imperative step to resuscitate free-market healthcare in the U.S. I wholeheartedly support HHS in its efforts to compel this much needed transparency from hospitals and medical providers. This will spur competition, lower prices and empower the patient to direct his or her own care. When providers and insurers enter into contracts claiming that the actual procedure pricing is "proprietary" and cannot be disclosed it hurts consumers, patients and the American economy in the form of inflated oligopoly pricing in healthcare. If we don't take legislative and regulatory steps like this to compel this broken market to reveal its actual pricing, America will default into socialized medicine because nobody can afford the perpetual 10 percent premium increases. People will throw their hands in the air and give up on the market if we don't help it heal with rules like these.
FN. 2: 45 CFR Parts 170 and 171, Section VIII, C., 3. found on Page 90 of 187 in this PDF:
Price Information
The fragmented and complex nature of pricing within the health care system has decreased the efficiency of the health care system and has had negative impacts on patients, health care providers, health systems, plans, plan sponsors and other key health care stakeholders. Patients and plan sponsors have trouble anticipating or planning for costs, are not sure how they can lower their costs, are not able to compare costs, and have no practical way to measure the quality of the care or coverage they receive relative to the price they pay. Pricing information continues to grow in importance with the increase of high deductible health plans and surprise billing, which have resulted in an increase in out-of-pocket health care spending. Transparency in the price and cost of health care would help address the concerns outlined above by empowering patients to make informed health care decisions. Further, the availability of price information could help increase competition that is based on the quality and value of the services patients receive. Consistent with its statutory authority, the Department is considering subsequent rulemaking to expand access to price information for the public, prospective patients, plan sponsors, and health care providers.
Increased consumer demand, aligned incentives, more accessible and digestible information, and the evolution of price transparency tools are critical components to moving to a health care system that pays for value. However, the complex and decentralized nature of how price information is created, structured, formatted, and stored presents many challenges to achieving price transparency. To this point, pricing within health care demands a market-based approach whereby, for example, platforms are created that utilize raw data to provide consumers with digestible price information through their preferred medium.
ONC has a unique role in setting the stage for such future actions by establishing the framework to prevent the blocking of price information. Given that price information impacts the ability of patients to shop for and make decisions about their care, we seek comment on the parameters and implications of including price information within the scope of EHI for purposes of information blocking. In addition, the overall Department seeks comment on the technical, operational, legal, cultural, environmental and other challenges to creating price transparency within health care.
Should prices that are included in EHI:
... The U.S. Department of Health and Human Services is seeking public comment on whether patients have a right to see the discounted prices in advance of obtaining care, federal officials said. The invitation for comment—outlined in a little noticed passage of a broader patient-data proposal released last month—is a major step toward a possible rule that could require providers to release such information, they said.
Commercial health-care markets are rife with complex systems of hidden charges and secret discounts. Policy makers, employers and patients are often unable to see clearly which hospital systems and doctor practices are driving high costs.
The administration’s vision—which would possibly include fines for noncompliance—is to arm patients with information needed to make health-care decisions much like shopping for other consumer services. Rates potentially could be posted on public websites, where consumers would check the negotiated price of a service before they pick a provider. That, in turn, could lead to lower copays or deductibles. ...
Insurers might demand the same hospital discounts won by competitors, while some hospital systems might push for payment rates that match their crosstown rivals’. If doctors’ negotiated rates become public, other doctors could lower their prices to try to lure away patients. ...
A group that advocates for patients praised the proposed rule.
“If this rule goes forward, it will be a huge step towards true pricing transparency and will finally allow patients to really see what their costs will be before a service—something that has rarely been possible before,” said Caitlin Donovan, director of outreach and public affairs at the National Patient Advocate Foundation, which advocates for quality health care for people with chronic, debilitating or life-threatening illnesses. ...
Administration officials could move to issue a final rule mandating the disclosure of negotiated rates after the comment period closes May 3.
The move follows a report on health-care markets issued in December by the Trump administration, which called for greater pricing transparency and cited reporting in The Wall Street Journal on the complexity of health costs, among other sources.
Regulators said the authority for requiring price disclosure stems from the 21st Century Cures Act enacted in 2016, which makes blocking of health information illegal under penalty of up to $1 million, and from regulations stemming from federal privacy law. ...
Fully forcing the rates into the open could change the dynamics of the health market. Employers and patients, given clearer comparisons, might change their habits—though consumers often show limited inclination to shop for health-care services, even when they face significant costs under high-deductible health plans.
“You can’t shop for care if you don’t know what the prices are,” said HHS’s Mr. Rucker.
Once publicly available, patients may have the benefit of third-party technology companies aggregating the price data and building shopping tools that show the negotiated costs for services charged by various hospitals and providers.
Out-of-network doctors could try to compete with in-network negotiated rates. Health systems that charge higher negotiated rates could lose business if they don’t match competitors’ rates or justify the reasons for their steeper costs. Employers could press their insurers to include hospitals with lower negotiated rates in their networks.
Hospitals are likely to push for insurers to be under the same transparency rules and be required to release the negotiated discounts they pay for patient care.I was on the Armstrong and Getty show the morning of March 11th to discuss this story:
“They’d need to bring insurers and payers into the equation because they have the data to determine for patients what their costs should be,” said Chip Kahn, president of the Federation of American Hospitals, which represents investor-owned community hospitals and health systems.
FN. 1: Sample Comment to Proposed Regulation - The language in Section VIII., C, 3 of this proposed regulation found on pages 90-91 of the PDF requiring medical providers to disclose the true pricing of medical procedures is an imperative step to resuscitate free-market healthcare in the U.S. I wholeheartedly support HHS in its efforts to compel this much needed transparency from hospitals and medical providers. This will spur competition, lower prices and empower the patient to direct his or her own care. When providers and insurers enter into contracts claiming that the actual procedure pricing is "proprietary" and cannot be disclosed it hurts consumers, patients and the American economy in the form of inflated oligopoly pricing in healthcare. If we don't take legislative and regulatory steps like this to compel this broken market to reveal its actual pricing, America will default into socialized medicine because nobody can afford the perpetual 10 percent premium increases. People will throw their hands in the air and give up on the market if we don't help it heal with rules like these.
FN. 2: 45 CFR Parts 170 and 171, Section VIII, C., 3. found on Page 90 of 187 in this PDF:
Price Information
The fragmented and complex nature of pricing within the health care system has decreased the efficiency of the health care system and has had negative impacts on patients, health care providers, health systems, plans, plan sponsors and other key health care stakeholders. Patients and plan sponsors have trouble anticipating or planning for costs, are not sure how they can lower their costs, are not able to compare costs, and have no practical way to measure the quality of the care or coverage they receive relative to the price they pay. Pricing information continues to grow in importance with the increase of high deductible health plans and surprise billing, which have resulted in an increase in out-of-pocket health care spending. Transparency in the price and cost of health care would help address the concerns outlined above by empowering patients to make informed health care decisions. Further, the availability of price information could help increase competition that is based on the quality and value of the services patients receive. Consistent with its statutory authority, the Department is considering subsequent rulemaking to expand access to price information for the public, prospective patients, plan sponsors, and health care providers.
Increased consumer demand, aligned incentives, more accessible and digestible information, and the evolution of price transparency tools are critical components to moving to a health care system that pays for value. However, the complex and decentralized nature of how price information is created, structured, formatted, and stored presents many challenges to achieving price transparency. To this point, pricing within health care demands a market-based approach whereby, for example, platforms are created that utilize raw data to provide consumers with digestible price information through their preferred medium.
ONC has a unique role in setting the stage for such future actions by establishing the framework to prevent the blocking of price information. Given that price information impacts the ability of patients to shop for and make decisions about their care, we seek comment on the parameters and implications of including price information within the scope of EHI for purposes of information blocking. In addition, the overall Department seeks comment on the technical, operational, legal, cultural, environmental and other challenges to creating price transparency within health care.
Should prices that are included in EHI:
- Reflect the amount to be charged to and paid for by the patient's health plan (if the patient is insured) and the amount to be charged to and collected from the patient (as permitted by the provider's agreement with the patient's health plan), including for drugs or medical devices;
- Include various pricing information such as charge master price, negotiated prices, pricing based on CPT codes or DRGs, bundled prices, and price to payer;
- Be reasonably available in advance and at the point of sale;
- Reflect all out-of-pocket costs such as deductibles, copayments and coinsurance (for insured patients); and/or
- Include a reference price as a comparison tool such as the Medicare rate and, if so, what is the most meaningful reference?
To the extent that patients have a right to price information within a reasonable time in advance of care, how would such reasonableness be defined for:
- Scheduled care, including how far in advance should such pricing be available for patients still shopping for care, in addition to those who have already scheduled care;
- Emergency care, including how and when transparent prices should be disclosed to patients and what sort of exceptions might be appropriate, such as for patients in need of immediate stabilization;
- Ambulance services, including air ambulance services; and
- Unscheduled inpatient care, such as admissions subsequent to an emergency visit?
How would price information vary based on the type of health insurance and/or payment structure being utilized, and what, if any, challenges would such variation create to identifying the price information that should be made available for access, exchange, or use?
Are there electronic mechanisms/processes available for providing price information to patients who are not registered (i.e., not in the provider system) when they try to get price information?
Should price information be made available on public websites so that patients can shop for care without having to contact individual providers, and if so, who should be responsible for posting such information? Additionally, how would the public posting of pricing information through API technology help advance market competition and the ability of patients to shop for care?
If price information that includes a provider's negotiated rates for all plans and the rates for the uninsured were to be required to be posted on a public website, is there technology currently available or that could be easily developed to translate that data into a useful format for individuals? Are there existing standards and code sets that would facilitate such transmission and translation? To the extent that some data standards are lacking in this regard, could developers make use of unstandardized data?
What technical standards currently exist or may be needed to represent price information electronically for purposes of access, exchange, and use?
Are there technical impediments experienced by stakeholders regarding price information flowing electronically?
Would updates to the CMS-managed HIPAA transactions standards and code sets be necessary to address the movement of price information in a standardized way?
How can price transparency be achieved for care delivered through value based arrangements, including at accountable care organizations, demonstrations and other risk-sharing arrangements?
What future requirements should the Department consider regarding the inclusion of price information in a patient's EHI, particularly as it relates to the amount paid to a health care provider by a patient (or on behalf of a patient) as well as payment calculations for the future provision of health care to such patient?
If price information is included in EHI, could that information be useful in subsequent rulemaking that the Department may consider in order to reduce or prevent surprise medical billing, such as requirements relating to:
- The provision of a single bill that includes all health care providers involved in a health care service, including their network status;
- The provision of a binding quote reasonably in advance of scheduled care (that is, non-emergent care) or some subset of scheduled care, such as for the most “shoppable” services;
- Ensuring that all health care providers in an in-network facility charge the in-network rate; and
- Notification of billing policies such as timely invoice dates for all providers and facilities, notwithstanding network status, due date for invoice payments by the prospective patient's payers and out-of-pocket obligations, date when unpaid balances are referred for collections, and appeals rights and procedures for patients wishing to contest an invoice?
FN. 3: Statutory Authority - HHS maintains that the authority for this regulation comes from "Section 4004 of the Cures Act added section 3022 of the PHSA (42 U.S.C. 300jj-52, 'the information blocking provision'). Section 3022(a)(1) of the PHSA defines practices that constitute information blocking when engaged in by a health care provider, or a health information technology developer, exchange, or network. Section 3022(a)(3) authorizes the Secretary to identify, through notice and comment rulemaking, reasonable and necessary activities that do not constitute information blocking for purposes of the definition set forth in section 3022(a)(1). We propose to establish seven exceptions to the information blocking definition, each of which would define certain activities that would not constitute information blocking for purposes of section 3022(a)(1) of the PHSA because they are reasonable and necessary to further the ultimate policy goals of the information blocking provision. We also propose to interpret or define certain statutory terms and concepts that are ambiguous, incomplete, or provide the Secretary with discretion, and that we believe are necessary to carry out the Secretary's rulemaking responsibilities under section 3022(a)(3)." This is located on page 85 in this PDF.
Interestingly enough, The 21st Century Cures Act was authored by a Democrat from Oregon and supported overwhelmingly by both parties. By in large, the law deals with health information technology protocols, information sharing, patient privacy, disclosure procedures, and a myriad of other health IT matters. That Act, directed HHS to basically determine what is and is not unlawful information blocking in the health IT realm.
The 21st Century Cures Act grew out of and expounded upon the HIPAA HITECH Law of 2009. That was part of the Obama Administration's Stimulus Package or the The American Recovery and Reinvestment Act of 2009 ("ARRA") That law passed congress almost entirely on party lines with only a handful of Republican politicians joining Democrats. Now, 10 years later, the Trump Administration is reaching deep within that legislative lineage to write this regulation.
FN. 4: Administrative law is an utter nightmare in America. We produce 60,000 to 90,000 pages of new rules and regulations in the federal register each and every year. Congress repeatedly abdicates its responsibility to legislate by passing broad, feel good, ambiguous measures and directing unelected administrative bureaucrats to write regulations that have the force of law. The phenomenon didn't even begin in the United States until 100 years after our constitution was adopted. There are very reputable law professors and scholars who maintain that it is either wholly illegal or at a minimum, has completely sprawled well beyond anything our forefathers could have imagined. For more on the extra-lawful sprawl of Administrative law into every aspect of our life, read and follow Tim Sandefur. I know of nobody better in America on the topic.
Hence, it is not without some trepidation that I find myself in favor of this proposed regulation. From a constitutional law perspective, my instinct is to reject all new laws and statutes unless those new mandates are narrowly tailored and necessary for a clear constitutional purpose like protecting our borders, right to bear arms or freedom of speech. Government force must be limited to the protection of the rights of individuals to life, liberty, and property. The government's proper role at this juncture in our history should be to repeal many of our duplicative, unnecessary and inane laws. The government should not interfere with two people's right to contract unless they are physically harming or defrauding another.
However, a government should also insert itself in the limited instances when markets fail to provide solutions. Whether those failures are for externalities like pollution or when the market perversion emanates from an arguably government-aided failure like in the case of monopolies and oligopolies. America's modern health insurance delivery system is a clear oligopoly with anti-competitive contracts built in to mask transparency. We are left with only four major, national insurance carriers in the U.S. The healthcare "market" has been choked off with hundreds of thousands of pages of statutes, case law and regulation in a mish-mashed attempt to partially socialize, protect the oligopoly's power and even help patients where that fits with the other two goals. It is broken and it cannot continue down its current path or we will end up with a fully socialized system within ten years.
So yes, it would be better for all of of us and it would be cleaner constitutionally if this proposed regulation had been clearly passed by congress. But it wasn't. And I'm in the trenches fighting the healthcare behemoth every day with American patients and businesses. So I'm willing to use whatever free-market tool is given to me and head into battle. I will not let pefect be the enemy of good in this struggle.
Tuesday, March 5, 2019

{kind=link}
Saturday, February 23, 2019
Friday, February 22, 2019
On Armstrong & Getty: Who Owns Your Healthcare Data? Our Guru's Info Will Blow Your Mind!
Insurance companies are gaining a ton of information about your health--and making predictions about you.
Is the information accurate? Who owns it? Who's profiting from it?
Listen to the Armstrong & Getty Extra Large Interview featuring Craig "The Healthcare Guru" Gottwals.
Incredibly alarming trend in our industry expounded on by Marshall Allen at Pro Publica / NPR:
Is the information accurate? Who owns it? Who's profiting from it?
Listen to the Armstrong & Getty Extra Large Interview featuring Craig "The Healthcare Guru" Gottwals.
Without any public scrutiny, insurers and data brokers are predicting your health costs based on data about things like race, marital status, how much TV you watch, whether you pay your bills on time or even buy plus-size clothing. ...
With little public scrutiny, the health insurance industry has joined forces with data brokers to vacuum up personal details about hundreds of millions of Americans, including, odds are, many readers of this story. The companies are tracking your race, education level, TV habits, marital status, net worth. They’re collecting what you post on social media, whether you’re behind on your bills, what you order online. Then they feed this information into complicated computer algorithms that spit out predictions about how much your health care could cost them.
Are you a woman who recently changed your name? You could be newly married and have a pricey pregnancy pending. Or maybe you’re stressed and anxious from a recent divorce. That, too, the computer models predict, may run up your medical bills.
Are you a woman who’s purchased plus-size clothing? You’re considered at risk of depression. Mental health care can be expensive.
Low-income and a minority? That means, the data brokers say, you are more likely to live in a dilapidated and dangerous neighborhood, increasing your health risks. ...
The industry has a history of boosting profits by signing up healthy people and finding ways to avoid sick people — called “cherry-picking” and “lemon-dropping,” experts say. Among the classic examples: A company was accused of putting its enrollment office on the third floor of a building without an elevator, so only healthy patients could make the trek to sign up. Another tried to appeal to spry seniors by holding square dances. ...
Robert Greenwald, faculty director of Harvard Law School’s Center for Health Law and Policy Innovation, said insurance companies still cherry-pick, but now they’re subtler. The center analyzes health insurance plans to see if they discriminate. He said insurers will do things like failing to include enough information about which drugs a plan covers — which pushes sick people who need specific medications elsewhere. Or they may change the things a plan covers, or how much a patient has to pay for a type of care, after a patient has enrolled. Or, Greenwald added, they might exclude or limit certain types of providers from their networks — like those who have skill caring for patients with HIV or hepatitis C. ...The full story is absolutely worth your time to read.
Friday, February 1, 2019
Thursday, January 17, 2019
Links: ERISA Lawyer Fees; Fake Health News; Canadian Care; HSAs & Obamacare Waste, Cost Explosions & Deaths
Momma, don't let your babies grow up to be lawyers ... unless it's ERISA lawyers ..."[T]he court found that hourly rates of $450 for the associate on the case and $900 for the partner to be reasonable and within the prevailing rates in the market of ERISA attorneys."
The IRS overpaid nearly $4 billion to Obamacare customers through tax credits last year, and because of the way the law is written it can't even try to collect on a quarter of that.
Remember the claim that the ACA was going to reduce the cost of healthcare $2,500 per family? Well, not so much. ObamaCare to Cost Large Employers an Added $4,800 to $5,900 Per Employee Per Year.
Government Healthcare: Nothing like a 60 hour emergency room wait for a hospital bed. But hey, it's free!
#FakeHealthNews: Burying the Lede ... Rand Paul is scheduled to have the outpatient operation at the privately administered Shouldice Hernia Hospital in Thornhill, Ontario.
It Sure Looks Like This Obamacare Program Has Led to More People Dying. Under the health law, Medicare started penalizing hospitals for too many readmissions. Now mortality rates are up.
Wellness programs — which provide financial incentives for healthy activities or preventive care — don’t work, as numerous studies have shown. Here and Here.
Hospitals are now required to post prices online. But most price lists are buried under many sub-menus or at the very bottom of a long page scroll. Nearly 75% of hospital websites in the study required three or more clicks to find the information. Some required 100s of clicks.
Cutting Employee Hours to Avoid ACA Requirements Costs Dave & Buster's $7.4 Million.
 With HSA changes, here's how to find your best option.
With HSA changes, here's how to find your best option.
The IRS overpaid nearly $4 billion to Obamacare customers through tax credits last year, and because of the way the law is written it can't even try to collect on a quarter of that.
Remember the claim that the ACA was going to reduce the cost of healthcare $2,500 per family? Well, not so much. ObamaCare to Cost Large Employers an Added $4,800 to $5,900 Per Employee Per Year.
Government Healthcare: Nothing like a 60 hour emergency room wait for a hospital bed. But hey, it's free!
#FakeHealthNews: Burying the Lede ... Rand Paul is scheduled to have the outpatient operation at the privately administered Shouldice Hernia Hospital in Thornhill, Ontario.
It Sure Looks Like This Obamacare Program Has Led to More People Dying. Under the health law, Medicare started penalizing hospitals for too many readmissions. Now mortality rates are up.
Wellness programs — which provide financial incentives for healthy activities or preventive care — don’t work, as numerous studies have shown. Here and Here.
Hospitals are now required to post prices online. But most price lists are buried under many sub-menus or at the very bottom of a long page scroll. Nearly 75% of hospital websites in the study required three or more clicks to find the information. Some required 100s of clicks.
Cutting Employee Hours to Avoid ACA Requirements Costs Dave & Buster's $7.4 Million.
 With HSA changes, here's how to find your best option.
With HSA changes, here's how to find your best option.
Subscribe to:
Posts (Atom)